Article topic: Pneumocephalus
Author: Amera Sadder, Sadeel Suwan
Editor: Hamzeh Aljarrah
Reviewer: Rahmeh Adel
keywords: Conservative treatment, Cushing triad, Mountain Fuji sign, Neurotrauma, Pneumocephalus.
Introduction
Pneumocephalus (intracerebral aerocele or pneumatocele) is a pathological collection of gas (mostly air) in the cranial cavity.1 The air may be within the ventricular cavities, brain parenchyma, subarachnoid, subdural or epidural space.2 It is classified into acute (less than 72 hours) or delay (more than 72 hours). Also, it can be classified as simple or tension pneumocephalus.3
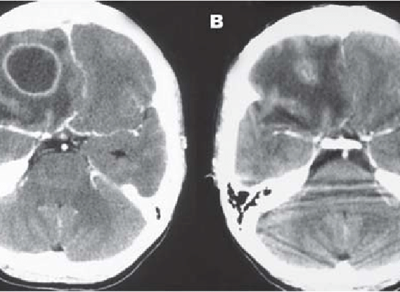
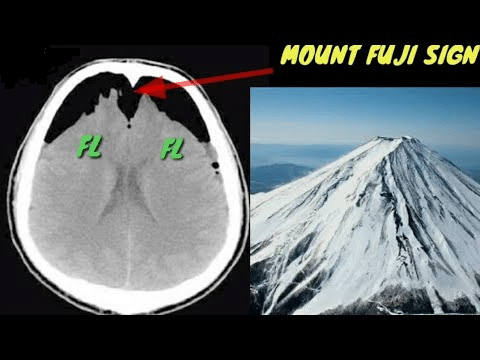
Tension pneumocephalus is intracranial parallel to tension pneumthorax 4 and is defined as an unceasing accumulation of intracranial air suggesting a “ball valve” causal mechanism, resulting in mass effect and compression of vital centers.5,6 The consequent signs and symptoms are unfortunately nonspecific and the diagnosis is confirmed by the appearance of “Mount Fuji” sign on unenhanced CT of brain.7,4 (Figure 1)
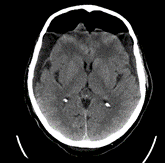
Figure 1: Pneumocephalus with Compression and Separation of Frontal Lobes
CT scan of the head. There is bifrontal pneumocephalus causing separation of the cerebral hemisphere, consistent with tension pneumocephaly with a Mount Fuji sign.7
Pneumocephalus and tension pneumocephalus share some causes like head trauma (especially skull base fracture) and neurosurgical interventions (lumbar arthrodesis is highly associated with pneumocephalus). Infections by gas-forming organisms (like Klebsiella pneumoniae 8) along with otolaryngeal procedures and diagnostic interventions (example: Lumbar puncture) can develop pneumocephalus, while epidural injections may develop tension pneumocephalus.1,4
Epidemiology
The demographic profile of affected individuals is linked to the underlying cause, with neurotrauma, particularly associated with skull base fractures, being the primary cause in 75% of cases. Despite limited epidemiological data, existing studies mainly consist of case reports.6,9 Traumatic head injury is the predominant cause of pneumocephalus, with its incidence ranging from 0.5% to 1% in head injury cases. Pneumocephalus can also emerge post-cranial surgeries or even spontaneously.6,10
Etiology
75% of pneumocephalus cases are attributed to neurotrauma such as skull basal fractures, penetrating injuries followed by dural lacerations, trauma of high pressure to the conjunctiva, fracture of air sinuses, and subarachnoid pleural fistula.11
The rest of the causes only compose the other 25%, which are congenital defects, infections, neoplasms, spontaneous, iatrogenic causes, and barotrauma.6,11
Congenitally like basal skull and tegmen tympani defects which cause spontaneous pneumocephalus due to Valsalva maneuver 12. Infections include meningitis and ventriculitis by gas-forming organism 8, sinusitis, or chronic otitis media. Neoplasms such as skull-eroding tumors like osteoma, epidermoid, pituitary adenoma, and dermoid cyst rupture. Spontaneous causes include CSF leakage from myelomeningocele, CSF fluid (rhinorrhea), and abnormal linkage between intracranial space and hyperpneumatized temporal bone.
Iatrogenic causes include ventriculostomies, positive pressure ventilators, transsphenoidal surgeries, endoscopic dacryocystorhinostomy or septoplasty, epidural or subarachnoid blocks, surgical site leakage, and spreading of subcutaneous emphysema through the ventriculoperitoneal shunt track into the brain6.
Pathophysiology
Pneumocephalus is the presence of intracranial air collection.5 Theories demonstrating the pathophysiology of pneumocephalus include the Dandy Theory of the ball valve (Figure 2) and the Inverted Bottle Theory (Figure 3) among others. Dandy theory of ball valve suggests a dural tear or a defect due to positive pressure ventilator, sneezing, or cough acts as a one-way valve (unidirectional air movement) thus trapping air intracranially.13,4
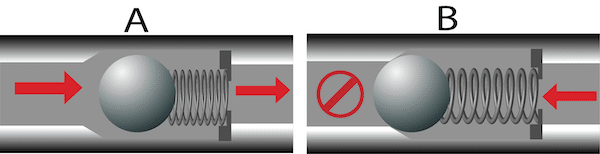
Figure 2: The Dandy theory of ball valve.
Spring loaded ball check valve in the open position allowing flow (A), and in the closed position preventing backflow (B)17
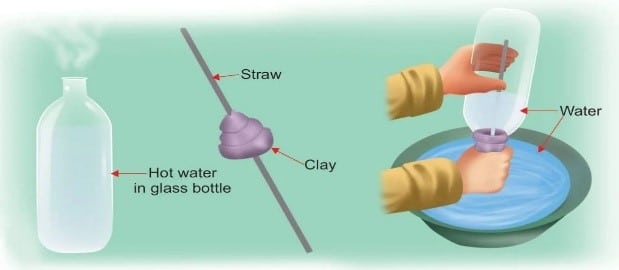
Figure 3: The inverted bottle theory.
The water in the bowl flows upwards against gravity into the bottle. This happens because of the hot air trapped inside the bottle. With the gradual cool down of the hot air, the
pressure inside the bottle begins to fall creating a vacuum in the bottle. It thus pulls up the water in the bowl through the straw.18
The inverted bottle theory implies that a vacuum is generated by excessive CSF leakage in the subarachnoid space resulting in the suction of air into the cranium until intracranial pressure equals atmospheric pressure. Trauma and surgeries are risk of developing dural tears which play a dual role, may cause CSF leakage (inverted bottle theory), or play as a valve (ball valve theory).1
Nitric Oxide in anesthesia can create or expand pneumocephalus since the blood–gas partition coefficient of nitrous oxide is 34 times greater than that of nitrogen, so it diffuses faster than nitrogen and air.14 Flights also have a role, the absolute cranial pressure decreases so air volume expands according to Boyle’s law, expanding pneumocephalus.15 (Figure 4)
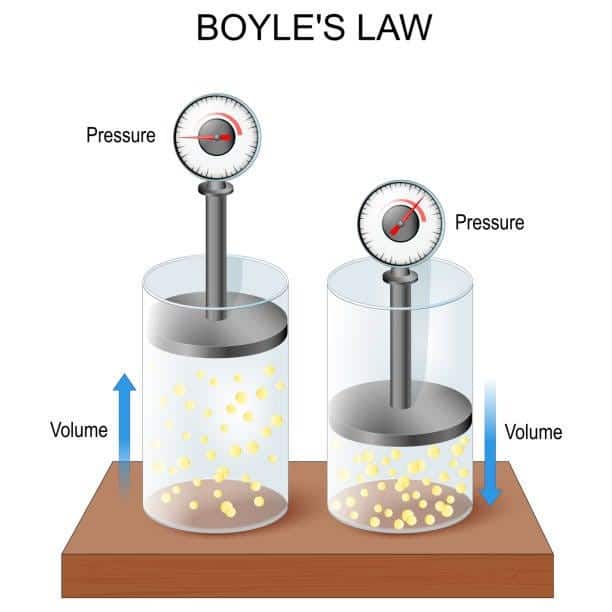
Figure 4: Boyle’s low.
It describes the relationship between the pressure and volume of a gas when the temperature is held constant. When the pressure decreases, the volume increases, and vice versa. 19
Pneumocephalus is rarely induced by gas forming bacteria and most patients have underlying infections like meningitis, subdural empyema, pneumonia or gastroenteritis. There is an interesting pneumocephalus case that was reported due to postoperative spinal wound infection by gas-forming bacteria (positive wound culture for C. freundii).1
Blowing the nose, coughing, or sneezing causes a sudden pressure increase in the air sinuses. Air is then drawn into the brain through defects in the skull base (Figure 5), used to identify the epidural space, is thought to be responsible for the development of pneumocephalus after epidural injections.6
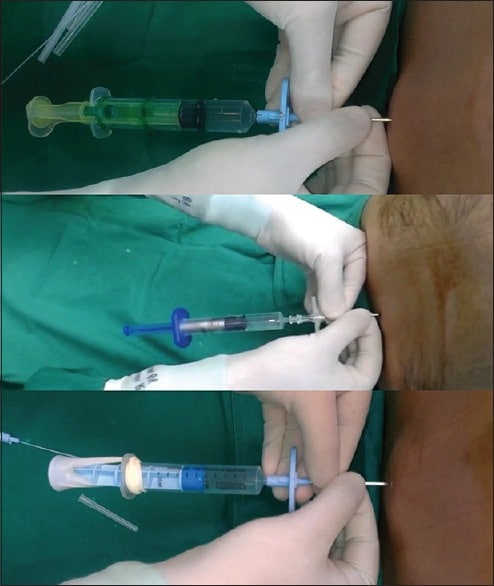
Figure 5: Epidural loss-of-resistance syringes, the Epimatic, the episure, and the modified syringe.20
Air entry through the meninges can be due to accidental injection, inadvertent dural puncture, or pressure gradients between the cranial cavity and atmosphere.6
Pneumocephalus is a benign and asymptomatic condition unless it induces mass effect with neurological deterioration.5 Air makes patients prone to infections like meningitis and can irritate the cerebral cortex causing seizures.6 Furthermore, rapid extra-axial compression of brain parenchyma contributes to severe neurological defects and fatal brainstem herniation.16
Clinical features
Pneumocephalus may be asymptomatic (due to spontaneous air absorption) or symptomatic.
An increase in intracranial pressure is the cornerstone of the symptoms, including nausea, vomiting, headache, dizziness, irritability, lethargy, and altered mental status ranging from drowsiness to coma. Additionally, it may be accompanied by CSF rhinorrhea 5, meningeal signs like nuchal rigidity 21, or surgical site infection like pain, swelling, and wound discharge.1 Moreover, cranial nerve defects like oculomotor palsy can occur.21 Rare presentations like frontal lobe syndrome, tinnitus, and flapping scalp signs were also reported.6
A patient with increased intracranial pressure may experience brain herniation, represented by the Cushing triad (hypertension, bradycardia, and irregular respiration) which may lead to fatal downward displacement of cranial contents.22
Diagnosis
Diagnosis depends heavily on detailed patient history (including past surgical, medical, and drug history), professional physical examination, and appropriate investigations.6
On physical examination, a rare splashing sound on head movement can be auscultated, known as (bruit hydro-aerique). Papilledema may be detected. Respiratory irregularities and cardiac arrest may be assessed if the posterior cranial fossa is involved.6
Computed tomography (CT) scan of the head is the gold standard for pneumocephalus diagnosis and can detect at least 0.55 ml of intracranial (IC) air. “Mount Fuji sign” which is the separation of the frontal lobes in supine position 7 (Figure 1), and the “Air bubble sign” pointed to the presence of multiple scattered air bubbles in several cisterns (Figure 6) are characteristic of tension pneumocephalus (Figures 7).17,18,19 A less severe condition is presented with a “Peaking sign” which means bilateral compression of frontal lobes with no tips separation (Figure 8).23
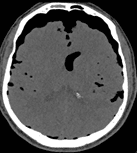
Figure 6: Air-Bubble Sign in Tension Pneumocephalus
CT scan of the head represents multiple small foci of air within the subarachnoid space, especially the Sylvian fissure. This air bubble sign is consistent with tension pneumocephalus.18
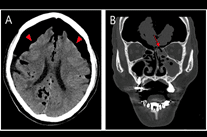
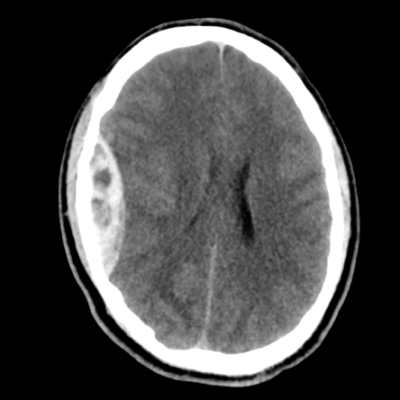
Figure 7: Tension Pneumocephalus
CT scan of the head. There is subdural air that causes a mass effect over the underlying brain parenchyma.19
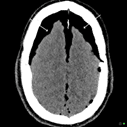
Figure 8: Peaked sign
CT scan of the head represents the frontal lobes being pushed together forming a peak in the midline giving a heaped-up appearance surrounded by air. Later, as the frontal lobes become separated they become the Mount Fuji sign.23
For calculating the volume of IC air there are two methods, one is by computer-assisted volumetric measurement and the other is the Bed-side technique; after selection a nearly central slide of the accumulated air, measure the maximum length “A” and width “B” in mm, then calculate the height “C” by multiplying the number of slides showing pneumocephalus with slice thickness. The estimated volume in mm equals AxBxC/2.624 (Figure 9)
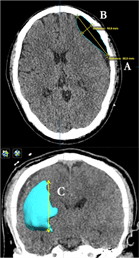
Figure 9: postoperative CT brain scan of chronic subdural hematoma with pneumocephalus.
The upper figure is for the ABC/2 method:
“A” is the largest longitudinal linear length of the pneumocephalus on the axial plane.
“B” is the maximum width from the inner table of the skull to the cerebral cortex perpendicular to A on the same slice.
“C” is the height of the pneumocephalus on a coronal plane, as determined by multiplying the number of CT scan slides with the pneumocephalus visible by the slice thickness (in this study, 5 millimetres (mm) in thickness).
The estimated volume was a multiple of A, B, and C and then divided by 2.
The lower figure is for the computer-assisted pneumocephalus volumetric measurement, semiautomatic segmentation was traced in each slice for computer-assisted volume calculation (lower) and 3D reconstruction of the pneumocephalus for visualization.24
Other imaging modalities like X-ray and Magnetic Resonance Imaging (MRI) can be used to detect pneumocephalus but they have limited sensitivity. In the latter, flow voids and blood products might be mistakenly interpreted for air, and X-ray detects at least 2 ml of IC air.6
Treatment
The primary treatment for pneumocephalus is conservative, aimed at preventing further air accumulation and complications. Key treatment strategies include keeping the patient in a horizontal or slightly elevated position to avoid worsening the condition. Positioning the patient at a 30° angle, known as the Fowler Position, helps evenly distribute air and prevents further accumulation. Patients are advised to avoid Valsalva maneuvers such as coughing, sneezing, or nose-blowing, which could increase intracranial pressure.25
Hyperbaric oxygen therapy (HBOT) is used to treat pneumocephalus by increasing the oxygen concentration in the blood, which in turn lowers the nitrogen concentration. This creates a gradient that facilitates the absorption of nitrogen from the air pocket in the cranial cavity into the bloodstream, reducing the size of the pneumocephalus.6,25
Continuous patient monitoring is essential to detect any complications or changes in the air collection. It is also common for patients to experience headaches within the first week after a craniotomy, affecting about 75% of individuals due to factors such as surgical manipulation, changes in intracranial pressure, and the presence of pneumocephalus.26
In situations where pneumocephalus leads to complications or symptoms, more aggressive approaches, such as surgical intervention may be necessary in cases of pneumocephalus when complications or symptoms persist despite conservative treatments. This is particularly true for tension pneumocephalus or instances where conservative strategies prove ineffective in preventing further air accumulation and addressing intracranial pressure. In such scenarios, more aggressive approaches become essential to mitigate risks and manage the condition effectively.11
Prognosis:
Pneumocephalus generally has a good prognosis with timely treatment, even in more severe forms like tension pneumocephalus. The most common type, simple pneumocephalus, often resolves on its own through conservative therapy, though it can occasionally cause seizures and meningitis. While tension pneumocephalus is more serious and can lead to complications such as paraplegia and hemiplegia, the outlook remains favorable with prompt and appropriate treatment.6
In most cases, pneumocephalus doesn’t cause symptoms. Tension pneumocephalus, a more serious variant, can lead to significant complications. Nevertheless, the overall prognosis for pneumocephalus is positive when timely and suitable treatment is administered. 27
Conclusion:
Pneumocephalus, often resulting from head injuries or surgeries, is an abnormal accumulation of gas in the cranial cavity. Classified into simple or tension types, it’s mostly asymptomatic and resolves with conservative treatment. Tension pneumocephalus can cause significant complications but with prompt treatment, the prognosis is generally good. Diagnosis is primarily via CT scan, and treatment focuses on conservative management, with surgery for more severe cases. Despite potential severity, timely and appropriate care typically leads to a favorable outcome.
References