Article topic: Alexia without agraphia
Authors: Raoul Al Kassis, Rita Kfoury
Editor: Omar Al Khatib, Joseph Akiki
Reviewer: Dr. Hala Qaryouti
Keywords: Alexia Syndrome Without Agraphia, Pure Alexia, Pure Word Blindness, Visual Verbal Agnosia
Abstract
Alexia without agraphia is a rare condition that should be distinguished from alexia with agraphia, where both reading and writing are significantly limited. It is most commonly caused by a cerebral vascular accident (CVA) or stroke at the level of the posterior cerebral artery (PCA). As a result, the splenium becomes infarcted. Depending on the degree of obstruction, some complications such as right-sided homonymous hemianopia and color agnosia could arise. Major symptoms that emerge after the onset of the disease are difficulty reading with intact writing ability and impaired vision. Alexia without agraphia syndrome is diagnosed by clinical examination and radiologic confirmation after ruling out serious visual or linguistic impairment. There is no proven cure but therapy can increase reading speed or letter recognition accuracy. Progression of alexia without agraphia is mostly governed by the nature of the underlying pathology. Some improvement is possible in stable lesions.
Introduction
Alexia without agraphia refers to a reading disorder in previously-literate individuals, most commonly occurring after a brain injury or stroke. The term alexia is derived from Greek and means ‘absence of reading’, distinguished from developmental dyslexia, which is a deficiency in learning capacities [1], and ‘alexia with agraphia’ which constitutes impairment in both reading and writing [2].
Also known as pure alexia or letter-by-letter reading, alexia without agraphia was first described by Dejerine in 1891 and 1892, when he detailed the symptoms of alexia and agraphia and attributed them to an injury in the left angular gyrus. He described it as an ‘acquired type of dyslexia’ [3].
After a brain injury, reading skills may be affected in different ways depending on the site and severity of the lesion, but the cardinal feature is a lack of reading comprehension. The patient’s ability to write, hear, and comprehend verbal language is intact. However, most cases present visual problems discussed later in the article.
Etiology
The most common reason is a cerebral vascular accident (CVA) or trauma leading to obstruction of the posterior cerebral artery (PCA) which affects different parts of the brain including the visual cortex. This is why this condition may be sometimes considered neuro-ophthalmological [4]. Other less common causes may include:
- Encephalopathy
- Surgery for a left occipital lobe vascular malformation
- Occipital tumors (e.g., glioblastoma) [7]
- Migraine, a rare cause of reversible alexia due to the compression of arteries [8]
- Multiple sclerosis [9]
- Epileptic focus [10]
“Congenital alexia” was also reported due to inflammatory or infectious processes (e.g., syphilis) [7].
Pathogenesis
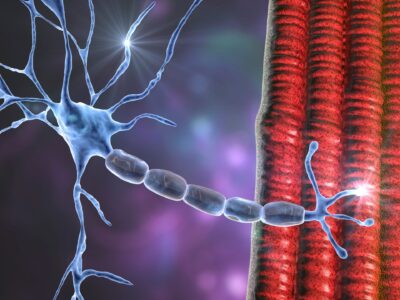
Figure 1 shows the parts of the normal brain responsible for conducting and possessing visual information into linguistic representations [14].
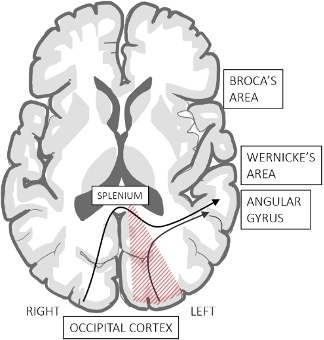
Figure 1: parts responsible for conducting and possessing visual information into linguistic representations
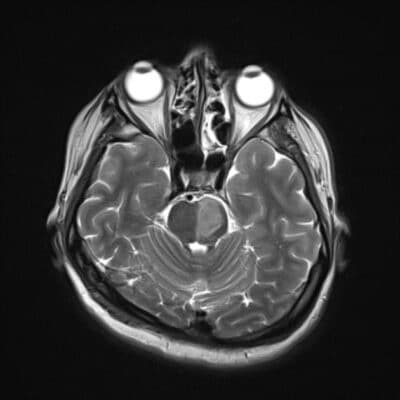
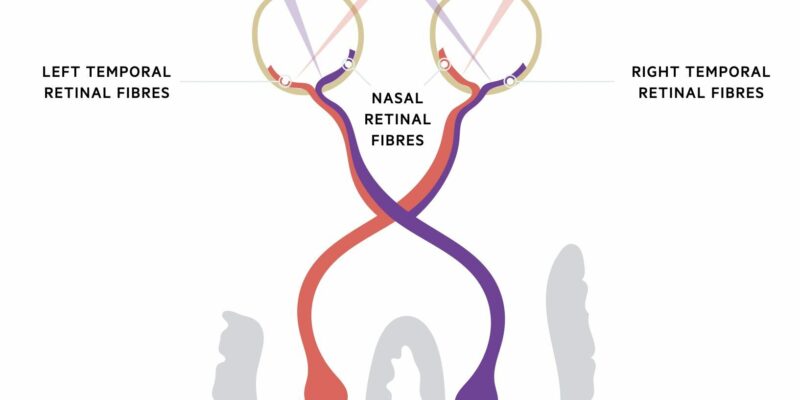
Figure 2 shows the visual pathways from the retina to the occipital lobe. Any lesion in this tract can result in partial or total blindness. Vision loss is represented below in red and blue [13].
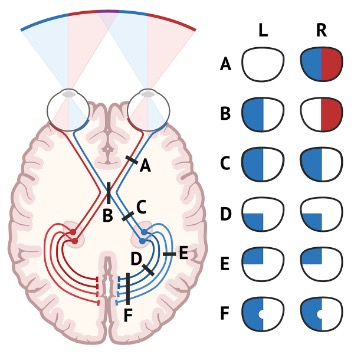
Figure 2: visual pathways from the retina to the occipital lobe
1. Normal Reading Process
The traditional neurologic reading model postulates functional connections between the left hemisphere’s angular gyrus and visual association regions in the occipital lobes.
The left angular gyrus is involved in translating visually presented input into linguistic representations, so it is mostly involved in reading and writing [5], thus, called the visual word form area (VWFA)[16]. On the other hand, the transfer of visual information between the visual occipital cortices and the left angular gyrus is done by the splenium (the posterior part of the corpus callosum).
2. Pure Alexia
In pure alexia, thrombosis of the left PCA results in infarction of the splenium and the left visual cortex, leaving the left angular gyrus intact [4]. Dysfunction of the left visual cortex will cause right-sided homonymous hemianopia [4]; a visual field defect involving the right halves of the visual fields of both eyes [6].
Infarction of the splenium impairs communication between the left angular gyrus and the intact right visual cortex, which only affects the connecting pathway. The angular gyrus is kept intact due to its supply by the middle cerebral artery, maintaining the patient’s writing ability [4]. In other words, the direct visual input to the left hemisphere will be blocked [13].
That’s why we attribute the term ‘disconnection syndrome’ to pure alexia since it is the connection pathways that are disrupted and not the visual word form area (VWFA) itself; unlike alexia with agraphia where lesion directly affects the left angular gyrus) [11].
3. Pure Alexia in Left-handed Patients
The VWFA is located in the motor cortex of the dominant hemisphere of the brain which is the left hemisphere in most people [23]. Studies suggest a direct correlation between handedness and the dominant side of the brain. Therefore, the dominant hemisphere of the brain is on the opposite side of the dominant hand in most cases.
For example, 27% of left-handed individuals have a right dominant hemisphere compared to only 4% of right-handed individuals with right hemisphere dominance [21]. So, a CVA on the right side of the brain, mainly in left-handers, could also be a cause of alexia without agraphia [22].
Clinical Presentation and Symptoms
The major symptoms and clinical findings include the following:
- Inability or poor, extremely slow ability to read words and phrases (4,17)
- Generalized malaise, confusion, and delayed response.
- Blurry vision and right-sided hemianopia.
- Intact ability to write.
- Equal pupils reactive to light
- Normal optic discs.
- Normal extraocular eye movements with no nystagmus.
- Intact language, sensory, and motor functions. [4]
- Short-term memory loss [15].
- Acute onset of headache and vomiting [18].
Table 1 further shows the effect on clinical aspects [15]:
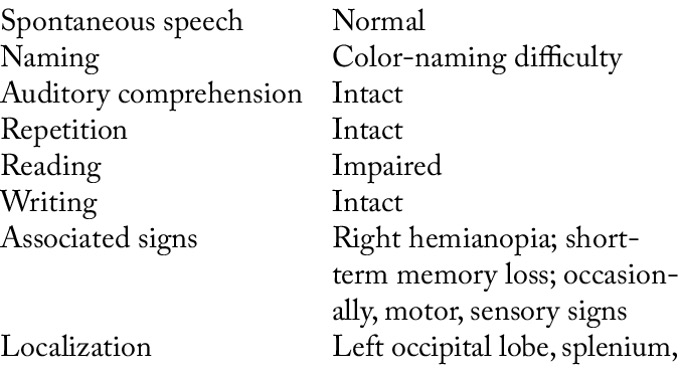
Table 1: clinical aspects
Complications
As previously mentioned, blockage of the PCA affects the left visual cortex which may lead to right-sided homonymous hemianopia. Patients may have visual concerns and seek ophthalmologic care, so an ophthalmologist should be aware of this neurological disorder. However, this complication is not always present [4].
Pure alexia may also present with or without color agnosia[19], which is the inability to identify and distinguish colors despite normal basic color vision and brightness discrimination mechanisms [20]. Depending on the severity of the CVA, more parts of the brain seem to be affected.
Diagnosis
Serious visual or linguistic impairment must be ruled out before making the diagnosis of pure alexia via clinical examination and radiologic confirmation [7]. To rule out agraphia, the patient is instructed to compose a brief paragraph [11].
Clear-cut cases are easily diagnosed by an attempt to read a little passage aloud. If the patient is unable to perform this, a simple letter or number reading is then attempted [11]. Particularly when the examiner is unsure of how to interpret the patient’s present reading skills in terms of their premorbid linguistic proficiency, a formal neuropsychological evaluation is essential in diagnosing partial or minor reading impairment [24].
Neuroimaging is crucial to determining the location of the lesion as well as to look for signs of pathology and point future investigations in the right direction. An individual with alexia and no lesion on an MRI scan has been reported to have hypometabolism in the afflicted area on an FDG positron emission tomography [25].
To distinguish a stroke from other etiologies such as abscess and tumors, a CT scan and/or MRI of the brain with and without gadolinium can be helpful. A typical MRI finding corresponds to a lesion of the left occipital lobe, due to the posterior cerebral artery’s vascular distribution [26,27].
The visual word form area, a region in the left lateral fusiform gyrus, has been linked in functional imaging studies to prelexical orthographic processing [28].
Differential Diagnosis
- Dyslexia: Alexia without agraphia is characterized by the loss of reading ability. This deficit sets it apart from the more well-known condition known as dyslexia, which is characterized by a delay in the development of reading competence beginning in childhood when most people learn to read [11].
- Bilateral ocular or cerebral acuity loss: Many aphasic conditions include impaired reading. Reading will be negatively impacted by a variety of visual impairments. Patients with bilateral ocular or cerebral acuity loss will have difficulty reading. Their acuity should be assessed using a nonletter optotype, ideally gratings, to prevent confusion [29].
- Bitemporal hemianopia: Reading can also be impaired by visual field problems that do not influence central acuity. Hemifield sliding may result from bitemporal hemianopia [29].
- Neglect dyslexia: It is a type of left hemineglect in which patients produce left-sided reading mistakes. They neglect the left side of lines and substitute or add different words on the omitted left side [30].
Whereas patients with hemianopia alexia have trouble reading the right side of words because of a right homonymous hemianopia brought on by a left PCA lesion [7].
- Left hemiparalexia: It is characterized by the absence of a homonymous hemianopic defect, an isolated splenic lesion may make it impossible to read the left side of a word [7].
- Acquired ocular motor apraxia: Unusual eye movements may make reading difficult. Reading can be substantially impaired by acquired ocular motor apraxia caused by bilateral frontal or parietal injuries [31, 32].
- Surface dyslexias: Central dyslexias are linguistically based reading disabilities. Surface dyslexics lack an internal dictionary and are unable to pronounce irregular words [33]
- Phonological dyslexia: Patients with phonological dyslexia have forgotten general pronunciation norms and are unable to determine how to pronounce fictitious words or unfamiliar words [34,35].
Treatment and Management
Although there are some signs that therapy can increase reading speed or letter recognition accuracy, no known treatments have been proven to help these patients read normally or even relatively fluently.
Pure alexia can be treated using a variety of vision rehabilitation procedures [7]. Treatment for patients suspected of having disconnection syndrome includes finger tracing of letters. Other modalities of treatment include altering the text to emphasize the spaces between words or phrases, improving oral articulation while reading, repeatedly reading aloud text, attempting to improve implicit or covert processing of whole words, and finger-tracing letters [11].
Patients with severe letter identification deficits are managed with tactile-kinesthetic training whereas multiple oral re-reading techniques may help more mildly impaired patients with deficits mainly reflected in reading speed [36].
Risk Factors and Primary Prevention
The most frequent risk factors are those that are linked to cardiovascular risk and can result in thrombotic or thromboembolic ischemic events [26]. For patients experiencing a PCA stroke that results in alexia without agraphia, evaluation, and management of any modifiable vasculopathy risk factors is advised. Patients with various etiologies should have care and preventative strategies focused on the root cause.
Prognosis
The progression of alexia without agraphia is mostly unknown. Most often the course is governed by the nature of the underlying pathology. Some improvement is possible in stable lesions [11]. No treatment has been proven to enable patients to read normally or near-normally [11]. Since no treatment or therapy significantly improves reading comprehension, strategies such as word-for-word reading, oral reading, and tactile and kinesthetic training are used to improve reading comprehension [7].