Article topic: Transient Global Amnesia (TGA)
Author: Rama Amourah
Editor: Haneen Al-Abdallat, Haneen A. Banihani
Reviewer: Ethar Hazaimeh
Keywords: transient, anterograde amnesia, retrograde amnesia, memory, venous insufficiency
Overview
In order to understand memory loss disorders, one must first understand memory itself. In the context of neuropsychiatry, memory is the ability to process, store, and recall or recognize information for subsequent use.¹ There are two large, interconnected categories for the type and longevity of information stored in human memory: short-term (or working) and long-term memory. Short-term memory can contain a limited amount of new information that can only be remembered for a brief period of time, whereas long-term memory allows an individual to store and retrieve an indefinite amount of information for an indefinite period. Repetition or processing of information in the working or short-term memory facilitates its conversion to long-term memory; conversely, if long-term memories are not retrieved, they may be forgotten.²
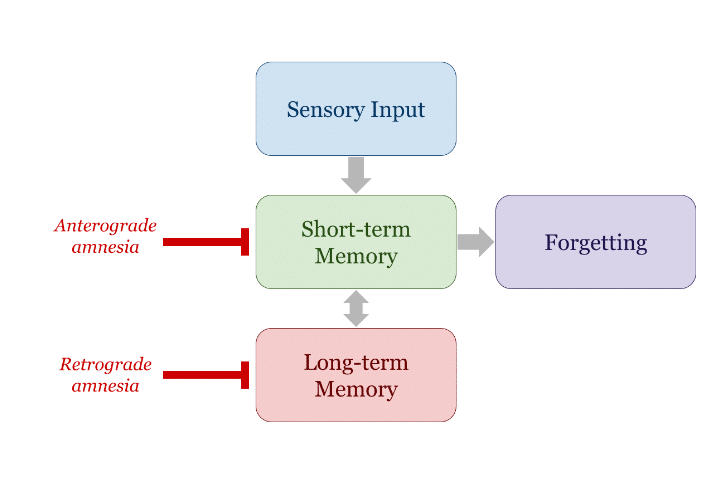
FIGURE 1: Flowchart of memory and amnesia¹̦²
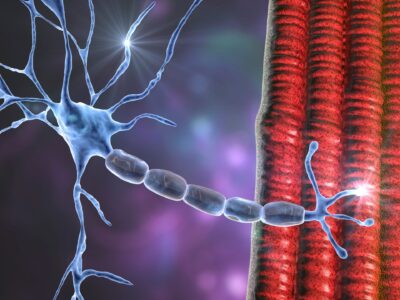
Amnesia is the transient or permanent loss of memory (the ability to store and recall learned information) without losing other cognitive functions. There are two types of amnesia: anterograde and retrograde. The difference between them is that people affected by anterograde amnesia cannot form new long-term memories due to an inability to commit information to long-term memory from short-term memory. In contrast, people with retrograde amnesia cannot recall previously formed long-term memories from a variable interval of the person’s life.³ People may acquire amnesia with anterograde and retrograde characteristics, which is described as global.²
Introduction
Transient global amnesia (TGA) is an attack of global amnesia that the affected individual fully recovers from within twenty-four hours. The presence of a trigger (such as emotional stress) and the deficit in long-term memory varies between patients, but what all cases of TGA have in common is that there are no other losses in cognitive and neurological function or associated signs and symptoms.⁴̦⁵
Etiology
The pathophysiology of transient global amnesia is disputed as of the writing of this article. Studies have proposed several different pathological processes which may cause this disease, which can be described as follows:
- Vascular
One of the theories is that TGA is caused by venous insufficiency, leading to an episode of venous congestion in the brain, particularly the medial temporal lobes.⁵ This could explain why many common triggers of TGA also increase intrathoracic pressure, increasing cerebral venous pressure (Figure 2).⁶⁷ Several studies found an association between TGA and internal jugular vein (IJV) valve insufficiency or occlusion of the brachiocephalic vein. However, other studies have found that IJV insufficiency does not explain all cases of TGA, and many people with IJV do not experience TGA.⁸ Another possible vascular cause for TGA is hypoperfusion due to arteriolar vasoconstriction in response to triggers, including hyperventilation and increased cerebral venous pressure. Several imaging studies have demonstrated that a significant proportion of TGA patients have imaging findings consistent with transient ischemia⁹; however, not all TGA patients have findings of cerebral hypoperfusion, and whether the ischemia is causative of TGA is unclear.¹⁰

FIGURE 2: Some common TGA triggers, sorted by frequency.¹⁰̦ ¹⁹
- Migraine-related
Migraine is most likely caused by cortical spreading depression: a cortical wave of neuronal hyperactivity followed by hypoactivity.¹¹ Cortical spreading depression or similar patterns of cortical neuronal polarization and depression have been implicated by some studies to be associated with TGA.¹² This is supported by the fact that people less than fifty-six years old who experienced TGA have a history of migraines.¹²̦¹³
- Epileptic
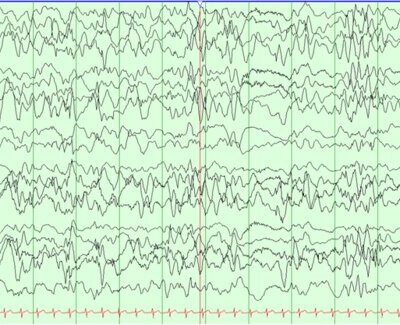
Some publications speculate that the pathophysiology of TGA is epileptic due to its similarity to transient epileptic amnesia (TEA), which is an episode of anterograde amnesia caused by an aware focal seizure of the temporal lobe. However, TGA and TEA are considered separate diagnoses with distinguishing features (Table 1), and studies found that patients with TGA have normal EEG readings.¹⁴
TABLE 1: Table comparing TGA and TEA.¹³
| TGA | TEA | ||
| Risk Factor | History of migraine | No | |
| Precipitating factor | Yes | Inconclusive | |
| Duration | Usually 4-6 hours, <24 hours | <1 hour | |
| Associated neurological symptoms | None | +/- Oral automatisms, gustatory and olfactory hallucinations | |
| EEG findings | No abnormalities | Abnormalities in temporal or frontotemporal areas | |
| MRI findings | Hippocampal DWI hyperdensity which resolves when the attack ends | +/- Hippocampal sclerosis or atrophy | |
| Risk of recurrence | Low | High | |
| Response to antiseizure drugs | Poor response | Responds well |
- Other
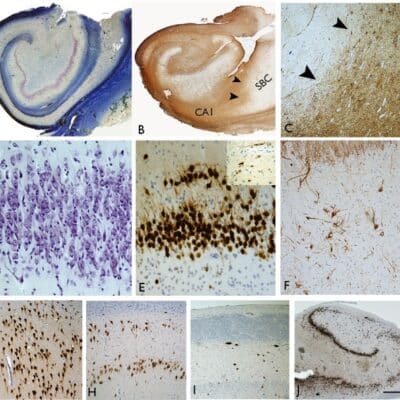
𝛃-amyloid deposits in the CA1 area of the hippocampus have also been found to be associated with TGA.¹²
Clinical Presentation
The typical TGA case is an adult approximately fifty to seventy years old who suddenly becomes disoriented to place and time and is distressed by this change. They often repeat the same questions, trying to orient themselves as to where they are and how they got to be in their situation. TGA patients may also have some degree of retrograde amnesia but are always self-aware and never present with other neurological or cognitive symptoms. The attack always resolves within twenty-four hours, and there is no change in the patient’s baseline neurological health.⁴̦ ¹⁰
Diagnosis and Investigations
TGA is a diagnosis based on the patient’s history and physical and neurological exam based on a set of criteria (Table 2). Imaging and other investigations are more helpful in ruling out differential diagnoses such as transient ischemic attacks (TIAs) and TEA than they are for identifying TGA.¹⁵
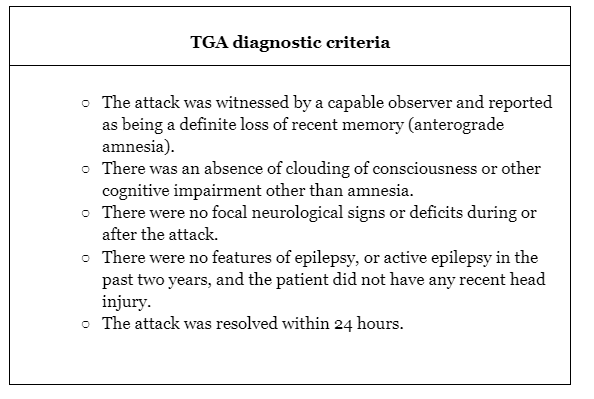
TABLE 2: TGA diagnostic criteria.¹⁶
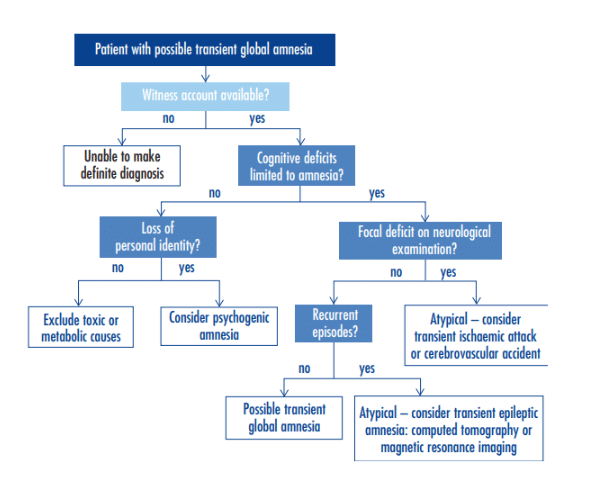
FIGURE 3: Flowchart for diagnosing TGA and its differentials.¹⁷
Treatment and management
TGA does not need treatment because it resolves entirely within twenty-four hours.¹⁸ It is essential to counsel the patient and their family about what happened and reassure them that TGA is benign.
Prevention
Given the low recurrence, low morbidity, and disputed etiology of pure TGA, there are few publications on preventing it.
Risk factors
People between the ages of fifty-six and seventy-five years old were found to have the highest occurrence of TGA. Most men who experienced TGA reported that it was preceded by physical stress, while women who experienced TGA reported emotional stressors and a history of anxiety or some personality disorder associated with their attack. People younger than fifty-six years old who had TGA are more likely to have a history of migraines than the general population.¹⁹
Prognosis
TGA has an excellent prognosis. Only 12.5% of people who experience TGA will have subsequent attacks, and their risk of TIA and dementia are 3% and 6%, respectively.²⁰ People who had TGA do not have a higher rate of vascular accidents, psychological disturbances, or mortality than a healthy control population, unlike people who experienced a TIA. That said, it is unclear whether or not TGA patients are at a higher risk of epilepsy and dementia than the general population.²¹
Recent developments
Researchers are exploring the possibility of a relationship between TGA and the SARS-CoV-2, or COVID-19, pandemic. A review of some case reports concluded that there had been an increase in the incidence of TGA since the onset of the pandemic; however, they were unable to conclude if that was due to the virus itself or the psychological stress of the pandemic.²²̦ ²³ Some publications claim that there may be an association between COVID-19 vaccines and TGA, but the link between the two is unclear.²⁴̦ ²⁵