
Article topic: Spinal Biomechanics and Basics of Spinal Instrumentation
Author: Yasser Banat
Scientific editor : Dr.Omar Jbara
Linguistic editor: Zain Alsaddi, phillip sweidan
Overview
The spinal column is a complex system that holds the spinal cord, nerve roots, and vertebral arteries. It is responsible for the transfer of electrical messages between the upper and lower limbs. This article will review the key concepts of spinal anatomy and physiology, energy transfer, the parameters of spinal alignment and also implant the properties required to plan a surgical procedure.
Spinal Anatomy and Physiology
The spinal column consists of three regions:
- The highly-mobile, lordotic cervical segment supporting the head
- The hypomobile, kyphotic, thoracic spine
- The mobile, lordotic lumbar segment, carrying 60-75% of the body weight.
The spine can be divided into the four following components: vertebral bodies (VBs), intervertebral (IV) disks, facet joints, and ligamentous structures (1).
The vertebral body, shown in Figure 1, is the main load-bearing structure of the spine. As the spine transitions caudally, the vertebral body’s width increases. This is due to the need for increased load-bearing. Moreover, The vertebral bodies are at their largest within the lower lumbar spine, so correspondingly can accept a larger pedicle screw diameter than the thoracic spine. (1)
The intervertebral disk is analogous to a shock absorber which acts on stabilizing the spine. Each disk is composed of a hydrated core of proteoglycans assembled in a loose collagen network called the nucleus pulposus and surrounded by a fibrocartilaginous ring called the annulus fibrosus to provide structural support.(1)
Facet joints perform two functions. They control the direction and amplitude of the axial movement and also share the load-bearing of the vertebral body. The ligaments of the spine provide stability. Bone-to-bone attachments provide tension and translational support (1).
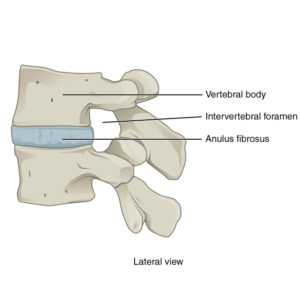
Figure 1: Lateral view of lumbar spine (2)
Pain and Energy Transfer
Trauma to the spine, whether acute or chronic, occurs secondary to excessive potential or kinetic energy that exceeds the absorptive capacity of the vertebrae and soft tissue, resulting in mechanical failure. Thus, failure of the normal spine or instrumented spine will occur if there is an energy transfer that exceeds the structural capacity of the spine and its construct. Pain in the lower back and neck is one of the most common medical problems in the adult population. (3)
Identifying factors that may increase the risk for or predispose individuals to developing back pain is important in attempting to reduce the prevalence and the social impact of this problem. Many studies have attempted to identify the contribution of multiple different demographic, physical, socioeconomic, psychological and occupational factors to the development of spine pain. Some of these factors are summed up in Box 1. (4)

Spinal Alignment Parameters
Postural changes play an important role in stress distribution across all segments of the spine. To meet the evolutionary demand of the upright posture, sagittal curves have evolved to distribute the normal physiologic loads applied to the spine. (7) There are three curvatures in the spine from cranial to caudal: cervical lordosis, thoracic kyphosis and lumbar lordosis.
- Cervical parameters: The lower cervical part is measured between C2 lower C7 endplates. The cervical spine may have lordosis, kyphosis, or could be neutral, depending on the value of the C7 slope.
- Thoracic parameters: Thoracic kyphosis is measured between the upper T1 endplate and the lower T12 endplate.
- Lumbar parameters: lumbar lordosis is measured between the point of inflection of lumbar lordosis to thoracic kyphosis and the upper S1 endplate. (8)
When the alignment is being evaluated, it is important to measure thoracic kyphosis, lumbar lordosis, and coronal curves on x-ray. Coronal curves are measured using the Cobb angle, in which an angle between the end vertebrae of a deformity is measured through the intersection of two lines parallel to the endplate of the superior and inferior vertebrae as in (figure 2). (5, 6)
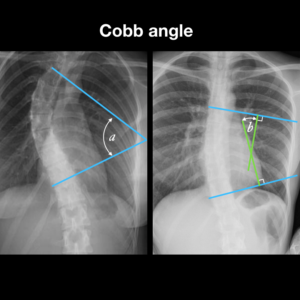
Figure 2: Cobb angle (6)
Kinetics and Kinematics
Studying kinematics is insufficient since it involves analyzing a subject’s motion without taking into account the underlying forces, wheras kinetics incorporates the subject’s mass and subsequent loading into the motion analysis to determine the relationship between the underlying forces and associated deformation. These results are expressed using the previously discussed curves. Whether designing implants or planning a surgical construct as a spine surgeon, it is important to account for the expected loading of the construct based on the local anatomy and patient’s parameters, such as weight and activity level. This planning is critical in preventing any implant failure. (9)
Implant Properties Required to Plan a Surgical Construct
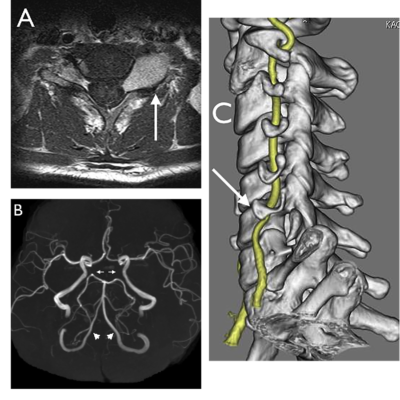
A spinal implant is a device that’s used to relieve back pain and manage disorders related to the spine as seen in Figure 3. They’re used to provide better pain relief, improve function and life quality as well as restore a long-lasting height for the vertebral body. (10)
Commonly used materials in spinal implants include stainless steel, titanium, and cobalt chromium, each having distinct properties. The two most important properties to consider are the stiffness and toughness or yield strength.
The choice of which spinal implant material to use depends on two key factors: patient bone quality and expected demands on a spinal construct. Bone quality is worse among: osteoporosis patients, elderly, renal disease patients, smokers, and osteomyelitis patients. (9) Implant failure results from fatigue through repetitive stress and strain to the implant.

Figure 3: Cervical spine implants (11)
Recent Study: The Effect of Sitting Posture on the Load on Spinal Joints
Since lower back pain is a common problem among most people, especially the ones who work in the office. A study was conducted to show the relation between the sitting posture and musculoskeletal diseases of the spine. It reported that people sit 8 hours a day. The pressure between intervertebral discs while sitting is twice the amount while standing. Figure 4 shows normal spinal curvatures.
The sample contained 20 students tested in three different postures, slump, lordosis and flat, to evaluate the moment and the AP (anterior-posterior) force on two main regions in the spine which are the cervico-thoracic and lumbo-sacral joints. The posture of the arms was taken in account as well (arms on chest, arms forward).
Results showed, the moment and the AP reaction force at both joints were much smaller in the lordosis and the flat postures compared to the slump posture. Also, the cervico-thoracic joint loads decreased in the arms-on chest posture. Consequently, flat or lordotic spinal curvature with arms near the axial line of the trunk is suggested to be a desirable sitting posture. (12)

Figure 4: Normal spine curvatures (13)




All the best wish you all success, good start