Title: Anterior Ischemic Optic Neuropathy
Author: Mohamad Srour
Editor: Odette El Ghawi, Joseph Akiki
Reviewer: Ethar Hazaimeh
Keywords: Anterior ischemic optic neuropathy, Arteritic Anterior ischemic optic neuropathy, Non-Arteritic Anterior ischemic optic neuropathy, Giant Cell Arteritis, Vision Loss.
Abstract
Background: Anterior Ischemic Optic Neuropathy (AION) is the leading cause of sudden vision loss in older adults. It is classified into non-arteritic anterior ischemic optic neuropathy (NAION) and arteritic anterior ischemic optic neuropathy (AAION). NAION is more common and is associated with systemic conditions like hypertension and diabetes, while AAION is linked to giant cell arteritis (GCA). The pathophysiology of NAION involves disrupted blood flow to the optic nerve head, whereas AAION is caused by vasculitis. Diagnosis is primarily clinical, with Optical Coherence Tomography (OCT) being crucial for differentiating between the two forms. The prognosis of NAION remains poor, with no proven effective treatment, although corticosteroids and antiplatelet agents are sometimes used. AAION requires prompt intervention with high-dose corticosteroids to prevent vision loss in the other eye. Despite these measures, the outlook for AION is often challenging. Recent advances have sparked interest in neuroprotective strategies and novel therapeutic agents, though these are still under investigation and not yet validated in clinical practice.
Methods: A comprehensive literature review was conducted using medical databases like PubMed and Google Scholar, focusing on key studies published between 2000 and 2024, with an emphasis on recent advancements and evidence-based practices.
Introduction
Anterior ischemic optic neuropathy (AION) is a sudden, painless loss of vision resulting from interrupted blood flow from the posterior ciliary arteries and/or ophthalmic artery to the optic nerve head [2].
Primarily affecting adults over the age of 50, AION can significantly impair visual function. This condition is broadly categorized into two types: arteritic AION (AAION), linked to giant cell temporal arteritis, a systemic inflammatory disease, and non-arteritic AION (NAION), which is more common.
Recognizing the symptoms and underlying causes of AION is crucial for prompt diagnosis and management, as early intervention can help prevent further visual deterioration and improve patient outcomes [3].
Figure 1 shows the anatomical blood supply of the orbit [1].
![Figure 1: Blood supply of the orbit [1].](https://neuropedia.net/wp-content/uploads/2024/08/Figure-1-Orbit-Blood-Supply.jpeg)
Figure 1: Blood supply of the orbit [1].
Etiology and Pathogenesis
Arteritic anterior ischemic optic neuropathy (AAION) is primarily associated with giant cell arteritis which affects medium to large arteries, particularly the temporal arteries. In GCA, inflammatory infiltrates in the vessel walls cause granulomatous inflammation, leading to luminal narrowing and reduced blood flow [4]. When this reduced blood supply affects the optic nerve head, it results in ischemia and subsequent vision loss.
Non-Arteritic anterior ischemic optic neuropathy (NAION) typically occurs due to acute hypoperfusion or insufficient blood flow to the optic nerve head, often triggered by nocturnal hypotension or systemic hypotensive events. This reduced perfusion causes infarction in the optic nerve head’s small capillaries, leading to ischemic damage and visual impairment [5].
Clinical Presentation
Patients with anterior ischemic optic neuropathy (AION) often experience a sudden, painless decline in vision, typically affecting one eye upon waking [6]. This rapid loss of vision is usually unilateral and may present with distinct visual field defects. An inferior altitudinal defect, characterized by a loss in the lower half of the visual field with a sharp horizontal border, particularly in the nasal periphery, is a strong indicator of AION [8]. Other visual field defects, such as central or sectoral losses, may also occur.
In the acute phase of AION, optic disc edema is a common finding, where the disc appears swollen, pale, and has a blurred margin [9]. Additionally, a relative afferent pupillary defect (RAPD) may be observed, where the pupil response to light is sluggish in the affected eye compared to the unaffected one [11].
In cases of arteritic AION (AAION), patients may also report systemic symptoms like headaches, scalp tenderness, jaw claudication, and polymyalgia rheumatica. A significant proportion of patients with GCA, up to 61%, present with AION at the time of diagnosis [10]. During fundus examination, disc edema is observed in approximately 64% of cases, while disc pallor is seen in around 49%, often accompanied by monocular or bilateral vision loss and headache [13].
Complications
Understanding the potential complications of AION is crucial for timely intervention, appropriate management, and mitigating the risk of further visual decline.
Permanent vision loss is a serious complication of AION, with many patients experiencing irreversible visual impairment in the affected eye, ranging from mild to profound. This sudden and significant loss can greatly impact daily activities, mental health, and overall quality of life [10]. Additionally, there is a risk of the second eye being affected, particularly in AAION, where bilateral involvement can occur if treatment is not promptly administered. In NAION, a second event in the fellow eye is possible, but the outcome remains unpredictable, with vision potentially being similarly or less affected [15]. Recurrent episodes of NAION can also occur in the same eye or the other eye, especially if underlying risk factors are not adequately managed. Over time, the initial disc edema typically resolves, leading to chronic optic atrophy.
Workup and Diagnosis
Clinical Evaluation
When evaluating a patient, it’s important to assess for sudden, painless vision loss, typically occurring in one eye[16]. Additionally, inquire about systemic symptoms such as headaches, jaw claudication, and scalp tenderness, which may indicate giant cell arteritis in cases of arteritic anterior ischemic optic neuropathy (AAION) [16-18]. During the physical examination, perform a thorough eye assessment, focusing on visual acuity and visual field testing. This should include checking for the presence of a relative afferent pupillary defect (RAPD) and inspecting the optic disc for signs of swelling or pallor [19].
Diagnostic Tests
- Fundoscopy: In the acute phase, optic disc edema and possible hemorrhages are observed. However, chronic cases may show optic atrophy with a pale disc [18].
- Visual Field Testing: Automated perimetry can identify characteristic visual field defects such as inferior altitudinal loss.
- Optical Coherence Tomography (OCT): Noninvasive OCT imaging measures structural parameters like optic nerve head morphology and macular details. It provides detailed information to assess disc edema and atrophy [18]. In addition, OCT-A can be useful in predicting the occurrence of AION in susceptible candidates based on its ability to measure the vascular parameters [20].
- Fluorescein Angiography: It helps in distinguishing between AAION and NAION by showing delayed or absent filling of the optic disc in AAION [20].
- Additional Tests: In cases of arteritic anterior ischemic optic neuropathy (AAION), elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels are common due to the underlying inflammation [21]. To confirm the diagnosis of giant cell arteritis, a temporal artery biopsy may also be performed [23].
- Imaging: MRI or CT scans of the brain and orbits may be used to rule out other causes of optic neuropathy, such as compressive lesions [25]. Additionally, 3D High Resonance MRI has been found to have a high specificity of 91% and a sensitivity of 70% in detecting giant cell arteritis-related ischemic optic neuropathy [23].
Differential Diagnosis
Optic neuritis is typically painful and linked to multiple sclerosis. It can be distinguished from anterior ischemic optic neuropathy (AION), which is generally painless and associated with systemic risk factors. Both conditions can cause sudden vision loss, but the presence of pain and a history of demyelinating disease point more towards optic neuritis.
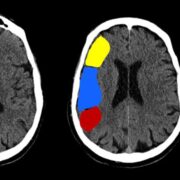
Figure 2 shows an example of left optic neuritis documented by T2 flair MRI [24].
![Figure 2: Left Optic Neuritis on T2/Flair MRI with effacement of the CSF within the optic nerve sheath [24].](https://neuropedia.net/wp-content/uploads/2024/08/Figure-6-Optic-Neuritis-300x300.jpeg)
Figure 2: Left Optic Neuritis on T2/Flair MRI with effacement of the CSF within the optic nerve sheath [24].
Other differential diagnoses related to optic neuropathy include diabetic papillopathy, inflammatory, infectious, and toxic causes [26-29].
Treatment and Management
Making timely interventions is crucial for improving visual and potentially vital outcomes. It’s important to increase awareness among non-ophthalmologist clinicians who may encounter these patients because most causes of acute ocular ischemia lack standardized treatment guidelines [32,33].
Arteritic anterior ischemic optic neuropathy
In the case of arteritic anterior ischemic optic neuropathy (AAION), immediate high-dose intravenous corticosteroids (e.g., methylprednisolone) are initiated to reduce inflammation and prevent further ischemic damage. This is followed by a transition to oral corticosteroids (e.g., prednisone), with a tapering schedule over several months, guided by regular monitoring of ESR and CRP [30]. Long-term follow-up is necessary to monitor for side effects of prolonged corticosteroid use, such as osteoporosis, diabetes, and hypertension [32-35]. Clinicians may also implement bone protection strategies, such as calcium and vitamin D supplementation, and bisphosphonates if needed [32, 34].
Non-arteritic anterior ischemic optic neuropathy
Treatment for non-arteritic anterior ischemic optic neuropathy (NAION) is limited and varies depending on the patient’s presentation. It primarily focuses on managing risk factors such as hypertension, diabetes mellitus, obstructive sleep apnea, and hyperlipidemia to improve vascular health. Low-dose aspirin may be prescribed to reduce the risk of further vascular events. In addition, it is advisable to avoid nocturnal hypotension exacerbation, such as by adjusting blood pressure medications to avoid nighttime dosing [36].
Although some studies have suggested that oral prednisone or erythropoietin might be effective in recent-onset NAION [24], a recent meta-analysis involving 32 articles for qualitative analysis and 6 articles for quantitative analysis found that none of the proposed therapies—steroids, steroids plus EPO, oxygen therapy, memantine, or levodopa/carbidopa—significantly improved visual fields or acuity [22]. While this remains controversial, some neuroprotective strategies aimed at preserving retinal ganglion cells, such as using neurotrophic factors, anti-apoptotic agents, anti-inflammatory treatments, and blood-optic nerve barrier stabilizers, have shown promise [21].
Providing low-vision aids and resources is also important to help patients adapt to visual impairment. Regular eye exams to monitor for changes in vision, involvement of the second eye, and assessment of risk factor control are essential.
Optic nerve decompression surgery was futile due to anterior NAION to its high adverse events intra and post-operatively (pain, diplopia, and central retinal artery occlusion), and its negative effects on visual acuity and fields [14].
Prevention
Early detection of giant cell arteritis (GCA) is crucial, as about 15-20% of patients with this condition develop arteritic anterior ischemic optic neuropathy (AAION). Prompt evaluation of symptoms such as headache and jaw claudication, followed by laboratory tests including ESR and CRP, and possibly a temporal artery biopsy, is essential for accurate diagnosis. Early initiation of corticosteroid treatment can prevent further complications associated with GCA [10-14].
Non-arteritic anterior ischemic optic neuropathy prevention is based on managing systemic risk factors. Hypertension, which affects 50-60% of NAION cases, diabetes (25-30%), and hyperlipidemia (40-50%) should be controlled through lifestyle modifications and medications [6, 9,10]. Treating obstructive sleep apnea (OSA), which is present in 70-80% of NAION cases, with CPAP therapy is also beneficial [2]. Smoking cessation and maintaining a healthy diet are additional important preventive measures [32]. Furthermore, the American Academy of Neurology (AAN) guidelines now recommend tailored antihypertensive therapy specifically to prevent nocturnal hypotension, highlighting the importance of individualized treatment plans in reducing this risk.
Risk factors
Non-Modifiable Risk Factors
Non-arteritic anterior ischemic optic neuropathy (NAION) predominantly affects males more frequently than females, with a ratio of 2:1 [19]. Age is a significant factor, with AION most commonly occurring in individuals over 50 years old and peaking between 70-80 years, while NAION typically affects those aged 50-70 years. Anatomical predispositions, such as a crowded optic disc, which is found in about 40% of NAION patients, can affect blood flow to the optic nerve head [9]. Additionally, NAION can occur in approximately 7% of patients with scleroderma [4]. Internal carotid artery dissection (ICAD) should be considered in younger patients, as it may cause ischemic optic neuropathy and can also be secondary to occult blood malignancy [1, 28]. Lastly, Psychogenic factors may influence angiogenesis regulation in AION patients [13].
Modifiable Risk Factors
Several modifiable risk factors contribute to the likelihood of developing AION:
- Hypertension: Increases the risk of optic nerve ischemia and is present in approximately 50-60% of NAION patients [9].
- Diabetes Mellitus: Exacerbates the risk and is seen in about 25-30% of NAION cases [9].
- Hyperlipidemia: Elevated cholesterol levels impact vascular health and affect 40-50% of patients [9].
- Obstructive Sleep Apnea (OSA): Associated with nocturnal hypotension, which can trigger NAION, and increases the risk by 3.98 times [2].
- Giant Cell Arteritis: Significantly increases the risk of AION and is found in 15-20% of patients [9].
- Smoking: A known risk factor for vascular diseases that may double the risk of optic neuropathies [9].
- Medications: Certain antihypertensives can exacerbate NAION risk by causing excessive drops in blood pressure during the night. Additionally, disease-modifying antirheumatic drugs (DMARDs) like methotrexate and immune checkpoint inhibitors have been linked to increased incidence of optic neuropathy [10, 6].
Addressing these modifiable risk factors through lifestyle changes and medical management is crucial for reducing the likelihood of developing AION.
Prognosis
About 50% of patients diagnosed with arteritic anterior ischemic optic neuropathy (AAION) experience significant visual deterioration, with a substantial risk of severe, permanent vision loss in the affected eye. Fellow eye involvement is common, but high-dose corticosteroid treatment can improve visual outcomes and prevent further vision loss. With prompt treatment, 60-70% of patients may experience some improvement or stabilization of vision [31].
In contrast, approximately 40-50% of patients with non-arteritic anterior ischemic optic neuropathy (NAION) suffer from some degree of permanent vision loss, and 20-30% may experience significant visual impairment. Vision recovery is generally limited, with only 25-30% of patients seeing some improvement. Many will have persistent visual deficits, and the condition can recur in the same eye or affect the fellow eye in 10-15% of cases, particularly if underlying risk factors are not managed. Subretinal fluid is commonly observed in NAION cases, and the volume of transudate at the optic disc, rather than retinal reabsorption dysfunction, is a key prognostic factor for visual recovery [30].
In the long term, both AAION and NAION can lead to chronic optic atrophy, which results in a pale, atrophied optic disc and persistent vision loss which can significantly impact a patient’s quality of life, affecting daily activities and mental health.
Management and early intervention are crucial for improving prognosis and minimizing visual impairment in patients with AION.
Recent Updates
Neuroprotective Agents for NAION
Trials investigating neuroprotective agents, such as intravitreal stem cell therapy and novel pharmacological agents, are ongoing. Preliminary results suggest potential benefits in preserving visual function, although conclusive evidence and FDA approval are pending.
RPh201 is a novel investigational drug that is being studied for its potential use in treating non-arteritic anterior ischemic optic neuropathy (NAION). It is a neuroprotective agent designed to target and mitigate the damage to retinal ganglion cells, which are crucial in the visual pathway and are affected in NAION. RPh201 looks promising as there were no reported safety concerns raised during its clinical trial phase 2a [26].
Another agent that is currently being investigated in the management of NAION is OS-Citicoline. In a human body model, OS-Citicoline treatment enhances neurofunction by improving retinal ganglion cell (RGC) function, neural conduction, and addressing visual field defects. This enhancement is achieved by supporting the metabolic needs of RGCs, promoting cellular repair, and improving neural signal transmission. Additionally, OS-Citicoline provides neuroprotection by maintaining or improving the morphology of the retinal nerve fiber layer (RNFL), which is essential for preserving visual function and preventing further damage in non-arteritic anterior ischemic optic neuropathy (NAION) [27].
Updated Guidelines
For patients diagnosed with AION, the European Headache Federation recommends the following [25]:
- Administer high-dose glucocorticoids in the acute phase when GCA is strongly suspected for 6-24 months, then tapering it according to response.
- Consider bone-sparing treatments like bisphosphonates, for patients on high doses of steroids.
- For confirmed GCA cases with refractory disease or comorbidities worsened by GC, consider the recently FDA-approved TCZ (Tocilizumab), an IL6 receptor antagonist.
- Use methotrexate as second-line therapy to maintain disease control and reduce glucocorticoids, though its effectiveness is mediocre.
- Consider aspirin therapy based on clinician discretion and patient preference, except where contraindicated by pre-existing conditions.
These recent updates reflect ongoing efforts to enhance treatment protocols and improve patient outcomes for individuals with AION.